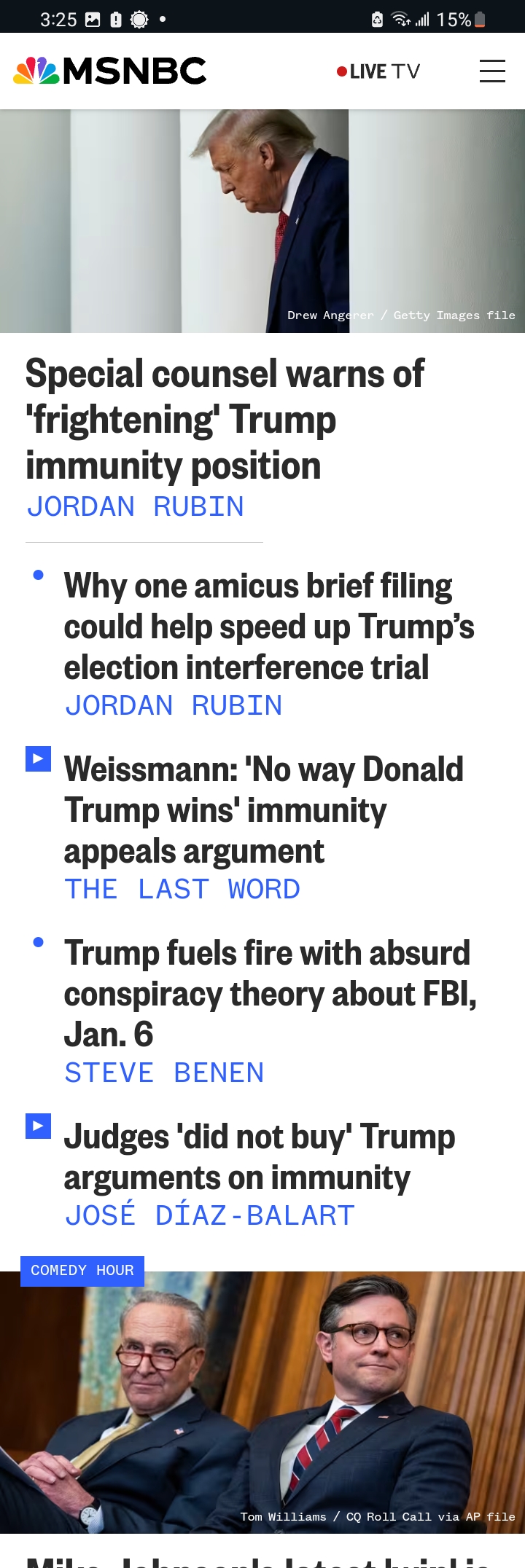
First and foremost, I really don’t have a political affiliation these days. My observations are without bias. That said, I took an interest in how much the MSM talks about Donald Trump, the former president of the US. It’s actually interesting as well as mind-blowing as to how much of the headlines are dominated by Trump–and have been for 8 years now.
I decided to log how many headlines are about Trump from the Big 5 outlets here in America. The log is from January 4, 2024 — January 11, 2024. Below, I have given the outlet for each day, and the number of headlines that are about Trump for each outlet over this 8 – day span of time. In total, there were 155 headlines about Trump combined within JUST 8 days. That’s honestly obsessive, because in my 44 years on earth, I’ve never seen the MSM give one man so much attention–good or bad–as Donald Trump.
Here is the log:
Jan 4, 2024:
CNN 1, ABC 2, Fox 0, MSNBC 5, NBC 3
Jan 5, 2024:
CNN 3, ABC 3, Fox 1, MSNBC 9, NBC 2
Jan 6, 2024:
CNN 4, ABC 1, Fox 2, MSNBC 6, NBC 3
Jan 7, 2024:
CNN 5, ABC 3, Fox 1, MSNBC 7, NBC 0
Jan 8, 2024:
CNN 3, ABC 5, Fox 2, MSNBC 6, NBC 4
Jan 9, 2024:
CNN 6, ABC 1, Fox 1, MSNBC 14, NBC 4
Jan 10, 2024:
CNN 8, ABC 2, Fox 2, MSNBC 8, NBC 5
Jan 11, 2024:
CNN 7, ABC 4, Fox 1, MSNBC 8, NBC 4
TOTAL: 155 HEADLINES ABOUT TRUMP
The times in which I recorded the number of headlines about Trump, taken from the BIG 5 MSM was conducted around 11:00 am — 2:00 pm daily for 8 days.
As everyone knows, the Israel-Hamas war is currently unfolding across the ocean, next to the Mediterranean. And here America is in the political division of the impact: Jews and Pro-Palestinians on the left side of the political sphere. Last week, there was a huge amount of coverages concerning the presidents of Harvard, UPENN and MIT. More than half of America wanted all three to RESIGN!
Not to mention, recently Harvard’s graduation included everyone but Jews. There was much exclusion within the realms of inclusion at the campus.
If one asked me if Harvard was antisimitic, I would have to say yes. The big question is: Why does Harvard choose to be antisemitic?
Some believe they take money from Qatar via donations, but I’m not too sure about that theory. Possibly, someone out there knows the answer to that rumor?
It doesn’t matter the reasoning, because antisimitism is wrong. Since when did we go back to the 1930’s in “progressive times”?
I must say, I have Jewish friends and I see their frustration concerning the antisimitism and nazism going on across the country. It’s not a pretty thing. I, personally am not religious, or of abt Abrahamic religion–but am spiritual. I do believe this war is a spiritual war, and America don’t want to swing antisimic, lest there’s hell to pay.
There have also been many attacks against Jews in the past weeks, from California to Massachusetts these attacks have occurred. And personally, I don’t agree with Biden’s silence in fear he’s going to offend someone. The game of identity politics is starting to dwindle, as people are waking up to how divisive they’re becoming.
In light of my ranting, antisimitism is very hypocritical and bad for America, politically and spiritually. All these years, America mostly has condemned Hitler and the holocaust–but now antisemitism is being embraced by a small sect of the leftist politics.
Liberalism is supposed to be about inclusion, and that’s something the hard left needs to reflect upon in combination to actually being Antifascists, because there’s nothing more fascist than siding with Hitler.
We need to condemn antisemitism before it first out if hand, abd the last thing Biden needs on his watch, is this situation to keep escalating. It’s bad enough what’s happened already is on his watch, looking back at everything in retrospect from the near abd distant future.
Furthermore, I have no political affiliation at this time. My thoughts and sentiments are not influenced by politics, but spirituality.
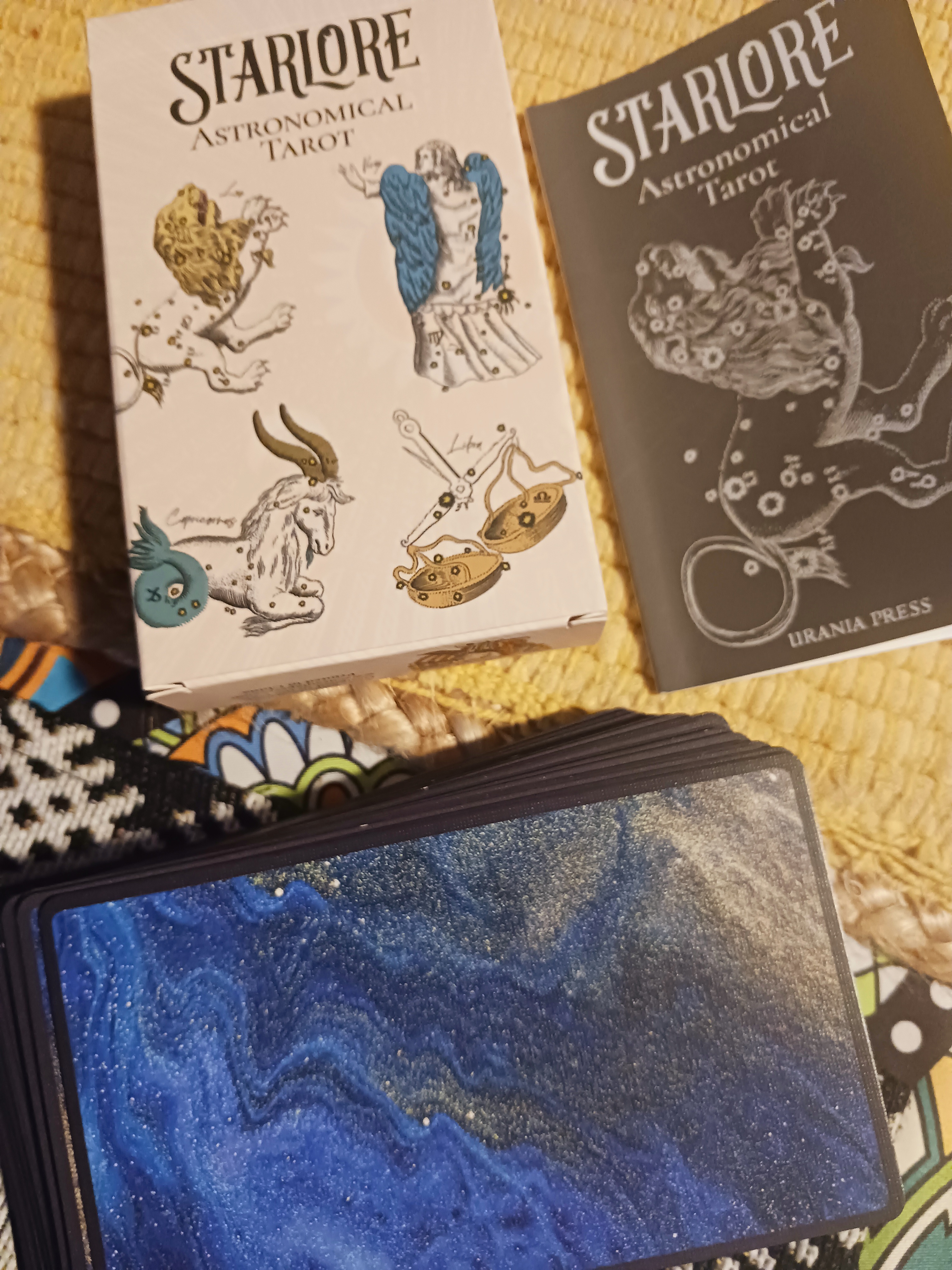
I have decided to blog about my new deck of tarot cards I purchased from an Etsy seller a few months ago: the tarot is rather differently from other decks, as this deck has an interesting take–a theme of constellations in combination with poker cards.
I have decided to start reading with the deck alongside my other decks. I find these cards beneficial regarding personal feelings of clients, and perhaps deeper insight into the minds and emotions of human psychology. I usually don’t use or go by manuals, so that’s a given that I won’t with this specific deck either. I usually assign my own meanings to each individual card.
Anyway, the first card I decided to scope and define is the VII of Hearts / Argo Navis:
Picture By: Billy Cahill
Taken from Google
After reading the history and legend above about Jason and the quest for the Golden Fleece along with a guided ship–we can automatically conclude the meaning of the card is our very own paths we walk, searching for something meaningful in life. However, given details of the card itself–we see the ship encompassed by some foggy cloud. This suggests, we must think clearly and with clarity of mind to reach our destination. life isn’t perfect, and more than likely, we’re not thinking too clearly along our path. All taken into account, it’s a good idea to inform the client, there’s indeed a choice and path that will be taken, but to think correctly, keep focus and meditate upon our new journey.
The card is rather a “mental card” that can, alone by definition mean: anxiety, turbulent times, depression, “road isn’t without obstacles “, mountain to climb, or perhaps a life lesson to learn all in retrospect, of course.
I’m going to share my turkey recipe. This recipe is my favorite, as it is the absolute best way to cook a turkey.
FIRSTLY, PLACE TURKEY IN PAN AND STUFF WITH 2 STICKS OF BUTTER INSIDE. NEXT, LAY ABOUT 5 MORE STICKS AROUND THE TURKEY IN ALUMINUM PAN–OR WHATEVER USED TO COOK TURKEY IN. 7 STICKS OF BUTTER IS FOR A 22 POUND TURKEY. THAT’S THE SIZE TURKEY I COOKED OVER THANKSGIVING.
NEXT, CUT UP FRESH WHOLE PINEAPPLE INTO SLUCES. PLACE A FEW SLICES OF PUNEAPPLE INTO TURKEY WITH BUTTER. PLACE ALL OTHER SLICES AROUND TURKEY WITH BUTTER.
NEXT COMES THE LEMON. CUT UP ONE OR TWO LEMONS AND PLACE THEM AROUND THE TURKEY WITH PINEAPPLE AND BUTTER. DO NOT STUFF TURKEY WITH LEMON. THE LEMON IS MOSTLY TO MOISTEN TURKEY, AND NOT FOR TASTE.
RUB ABOUT 3 TSPNS OF THYME ON TURKEY. ALSO RUB SALT AND PEPPER ALL OVER TURKEY.
FINALLY, POUR ABOUT 1/2 CUP OF OLIVE OIL ONTO AND AROUND TURKEY. NEXT, POUR A FEW CUPS OF WATER AROUND TURKEY INTO PAN.
NOTE: THE COMBINATION OF ALL THESE INGREDIENTS MAY NOT SOUND TOO TASTY, BUT WORRY NOT! ONCE EVERYTHING COOKS ABD BAKES TOGETHER, YOUR TURKEY WILL COME OUT SUPER DELICIOUS AND MOIST. THE PINEAPPLE AND LEMON MAKE THE TURKEY SUPER MOIST AND DELICIOUS. THEY DON’T LEAVE MUCH OF A SWEET OR BITTER TASTE ON TURKEY AT ALL.
AFTER PREPPING THE TURKEY, I COOK THE TURKEY OVERNIGHT AT 250 TO 275 DEGREES.
I thought I would blog about tarot becoming therapeutic for the spirit and soul. Understand I do believe in God and Christ (Major and Minor Sphere), spiritually. All said, I would never try to replace the trinity or anyone’s spiritual beliefs with JUST tarot cards for the spirit alone. My intention is to share free-flowing words abd thoughts on tarot.
Tarot has helped me significantly in the realm of understanding, philosophy, intuition and centering myself. I was sick some of this year, and tarot really helped me get through some bad times. Shuffling, casting and meditating on tarot n combination with God would feel me with a natural “feel good” energy–enlightening myself and illuminating my journey ahead. The cards are not all positive (X of Swords, Tower and so on) but I know life isn’t all cupcakes and lollipops. Sometimes we need obstacles in our way in order to grow, strengthen and enlighten ourselves. By all means, I am no guru, but I do like sharing my experiences–even if they’re small and sentimental.
I am a tarot reader of 30 years. I started reading back in the 90’s as a teenager, and looking at the BIG picture (retrospect), I can say tarot has been a big part of my life. I highly recommend them as spiritual therapy or a widening of the mind.
If you’re looking for self-advice and a place to start your journey–I recommend tarot as a sort of ignition. There are many other tools out there for therapy and starting your own personal journey . . . but take tarot into consideration.
Dealing with depression is something we’re all familiar with in one way or the other. That said, some of us deal with it on some other extreme levels. I personally don’t deal with it constantly, but I do have “bouts” or “tides” of it. The stresses and pressure of the world doesn’t help either. The only thing I can do is wait it out. Of course with my depression comes insomnia; it’s a rather nightmarish scenario.
So, the first coping skill I’ve learned is to think of the future, and perhaps a better day, week, month or year is approaching. Surely, something will get better–or some optimistic outlook can be had.
The next coping and therapeutic skill is what I do. I’m a tarot reader, and I do enjoy what I do. It gives me a reason to feel appreciated or useful to society. I understand society can be skeptical of my realm of work, yet that doesn’t have any impact on what I do. I still find some reason to live, obtain philosophical understanding–and know I helped someone with their life. All and all, I find my work therapeutic to my off and on depression.
The last coping skill I’ve learned is calmness, coziness and tranquility all within the moment and hour. To remain grounded and as clear minded as possible within present time. I try to understand and realize, whatever it is fueling anxiety and depression perhaps isn’t as bad as I make it. I try surrounding myself with comfort, candles and solitude. It doesn’t always work, but when it does–I find it necessary and therapeutic.
Picture taken in Eden, NC, Nov 2023. Sunset out in the country.
Everyone who struggles with some form or type of depression varies. Understand, my advice is what helps me. It’s definitely not for everyone. My dx was bipolar, but my bipolar is not as bad in severity as some others. My bipolar stems from some neurological mishaps from my early 30’s (now 44). Of course, I’ve tried many medications from Buspar, Trazadone, Risperdal, Zyprexa, Paxil, Klonopin, Lithium and Tegretol. None really helped in the long run. Some can benefit from medication, but I wasn’t really one of them. So, I have to find other ways to cope with my rollercoastering ups and downs throughout time and intervals.
On another note, depression can stem from life itself. I personally believe there is such a thing as “developmental depression” or a depression that can come on as we age. Getting older, not a soul relishes. That said, it is part of life, and cannot be avoided. To watch our loved ones get older is depressing. The thoughts of something happening to them is, in itself depressing. The grieving of losing your youth is depression, and how you’re going to keep ageing without remorse can be depressing, so on….
All said and the point taken, life itself can take a toll on how our depressions thickens over a course of time. If it isn’t dealt with, stress settles in–and it makes life an utter hell.
Coping us important, and coping is individualized. My coping skills may not be any use or beneficial for someone else’s depression. Understand my depression is mild in comparison to x, y or z’s depression. However, my story and babbling may be useful to someone out there. People need to understand and acknowledge they’re not alone, and that’s the real overall meaning and purpose of my blog entry.
Picture By: Billy / William Cahill (myself with crystal ball prop)
So, we come to ask what does 2024 have in store for the world. I personally feel something prophetic and radical in the air. It is by natural instinct, I believe we are in a time that’s been rather stagnant, and change is on the way. The hard truth is these changes aren’t so easy to grasp or live through. I see some major destruction that will occur along a river. There will be crying, restlessness and communities pulling together to help the poor and lonely. Candlelight vigil followed by comfort will occur.
It’s no coincidence this eclipse is powerful in contrast to the closing of the one that occurred in 2017. I figure these two eclipses (7 years apart) have meaning–spiritually, physically and prophetically. They do! Some odd events will follow this omen, yet all is by reason. Times will change and people will have to adapt with these changes. Of course, my visions run from April, 2024 to February of 2031.
There will be some great quakes that will occur along with adaptation, yet these changes within specific country will mark some change and revolution. The politics will change as well, and this will also start another chapter in time. As a humanity, challenges are needed to grow and eventuate into actual unity instead of imitation.
All is spiritual, and not easily understood. One day soon, we will understand and it is expected by us to understand via spiritual forces and realms up high and concealed.
So, what does Thanksgiving mean to you? Thanksgiving can mean many things to many people. The outlook on the holiday can be individualized concerning how people interpret and see it. It’s that time of the year, where a spirit of past, comfort and abundance comes together with family–or even by yourself. That feeling of coziness and wholesomeness surrounds the table as delicious food decorates it.
I’ve lived through 44 Thanksgivings, and each one has been so different. Last year, I was sick but recall celebrating abd eating anyway. This year, my mother was with us for Thanksgiving. I’m very happy to have spent this holiday season with my mother. However, it just wasn’t about spending time with mom, but to enjoy life while we have it.
The feeling of comfort, candles, food and the overall spirit of the season itself entered into my very temple as the days last two weeks went by in a hurry. Doesn’t time always fly looking back? And therein is why I relished and enjoyed the moment of Thanksgiving.
I even tried a different recipe for my turkey this year: I used pineapple, lemon, thyme, salt and pepper on my turkey. Also 7 sticks of butter stuffed within to keep it moist. The turkey came out delicious.
Thanksgiving this year was very delicious and wholesome.
I hope everyone had a pretty good holiday and cherished the moment.
All this said, my heart was with all those suffering war between Ukraine and Russia, Israel and Palestine. It’s hard to push the less fortunate away out of your mind, when you are celebrating and know there’s people and children out there enduring such heartache and suffering. It’s only human to care and pray for those who are in need.
All and all, the best and worst of times will one day be a distant memory–from another realm and perspective.
Back in April of this year, we decided to take a trip to New Orleans. I had never been there, and decided it was time to go. It was rather a fun trip, in spite of me being sick with some neurological problems.
There was so much to do, from dining to enjoying the history, taking in the vibes, shopping at nifty and occultistic shops here and there–and listening to jazz.
I did get the opportunity to stop at the VooDoo Museum. It was rather small, but packed with history that seem to be nearly forgotten by some in the modern world. The museum and vibe was like a mixture of cultures from French, African Creole and a splash of catholicism. I really enjoyed my visit to New Orleans, and was very enlightened by the experience.
It has been a while since I have blogged. My life has been super busy traveling, giving tarot readings and just…”living”. It’s a pretty mundane life, yet interspersed with entertainment from time to time.
A few nights ago, I took a picture of the Lunar Halo, which seem to mark some new beginning of time–you could say. It’s almost as if something changed in the flow of how life was, well, flowing…
May these vibes be positive and enchanting, bringing a new era of my life. I personally believe 2024 will be a challenging year, globally. That said, a year that will bring some much needed to change to us all.
AND I’ve learned by the age 44, we go through struggles (individually or collectively) in which at the same time presently we feel weak, tired and close to giving up. That said, always in hindsight, it’s for the best we endured and fought to the end like lions and warriors. That’s 2024 in a nutshell.
We must also take into account the upcoming eclipse in April, and some catastrophe following it. Astronomically and Astrologically, these are challenges tied together with prophecy.
BUT WE WILL ENDURE. We will overcome! We will be polished and enlightened by hard lessons as an individual–or together.